Key Takeaways
- GDNF stimulation: Ibogaine and its metabolite noribogaine may upregulate glial cell line-derived neurotrophic factor (GDNF), a protein that protects and repairs neurons.
- The 90-day window: Research suggests noribogaine reopens neural plasticity in the months following treatment, offering a critical window for integration work and rehabilitation.
- Clinical evidence emerging: DemeRx's Phase 1 trials of oral noribogaine (DMX-1001) showed positive results in 55 UK participants; Ambio's case study documented functional improvements in a 43-year-old with Parkinson's.
- Mechanism diversity: Unlike single-target drugs, ibogaine acts across multiple brain receptors, potentially addressing the complex biology of neurodegeneration.
- Integration matters: The medicine alone is not the cure. Nutrition, movement, meditation, and cognitive work during the neuroplasticity window appear essential to lasting change.
- Not a clinical recommendation: This article explores emerging science. Anyone considering ibogaine-assisted therapy should consult qualified medical professionals and understand local legal status.
The Question That Doesn't Leave
You wake up, and the first sign appears again: tremors, a word that won't come, a balance that's shifting. Or you're watching someone you love—a parent, a partner—slip further each month. The doctors say there's no cure, only symptom management. So you search. You read. You wonder: Is there anything else?
For some people exploring neurodegenerative conditions, that search leads to ibogaine. Not as miracle. Not as replacement for medical care. But as a name emerging in research—one that whispers differently than the others. And the whisper is worth understanding.
What Ibogaine Does: Beyond the Obvious
Ibogaine is a complex alkaloid from the African iboga plant. It doesn't work like a typical pharmaceutical. Rather than targeting one receptor or one pathway, ibogaine engages multiple systems across the brain—serotonin, dopamine, glutamate, NMDA, sigma receptors, and others. This complexity, once seen as a drawback, is increasingly understood as a feature.
When ibogaine is metabolized in the body, it becomes noribogaine—a compound with a particularly long half-life and a different receptor profile. Research by Dr. Deborah Mash and others suggests noribogaine may be responsible for some of ibogaine's most interesting neuroprotective and neuroplastic effects.
The GDNF Connection
One of the most compelling threads in the emerging research concerns GDNF—glial cell line-derived neurotrophic factor. This is a protein that nourishes dopamine neurons, the very cells that die in Parkinson's disease. GDNF is also involved in broader neuroprotection, supporting nerve growth and preventing degeneration in multiple neurological conditions.
Several preclinical and early clinical observations suggest that ibogaine and noribogaine may upregulate GDNF expression. In other words, the medicine may signal the brain's own repair mechanisms to activate. This is fundamentally different from adding a chemical to replace what's lost—it's more like waking up the body's own healing capacity.
Beyond GDNF, the neuroplasticity reactivated by noribogaine appears to unlock broader mechanisms of neural repair—neurogenesis, synaptogenesis, and the structural remodeling of circuits damaged by degeneration. This is the foundation for the 90-day window phenomenon discussed next.
The 90-Day Neuroplasticity Window
One of the most intriguing findings in ibogaine research concerns timing and neuroplasticity. After ibogaine treatment, research suggests the brain enters a heightened state of plasticity—a window during which neural pathways can be rewired, new connections form more readily, and rehabilitation efforts may have outsized impact.
This window appears to be roughly 90 days. It's not infinite. It's not guaranteed. But for those who have worked with the medicine, this period is often described as a second chance—not to reverse years of neurodegeneration, but to arrest it, redirect it, rebuild around it.
This is why the work after the medicine matters so much. The medicine opens a door. What you do in those 90 days—the movement, the nutrition, the cognitive work, the meditation, the integration—may determine what that door leads to. Research and clinical observation suggest that this window is not infinite, but it is actionable.
Clinical Evidence: What's Actually Happening
DemeRx Phase 1 Trial: Noribogaine DMX-1001
Dr. Deborah Mash founded DemeRx to advance noribogaine as an oral therapeutic. In 2024, the company announced positive results from a UK-based Phase 1 multiple ascending dose study with 55 participants. While Phase 1 primarily measures safety and tolerability, early signal data matters.
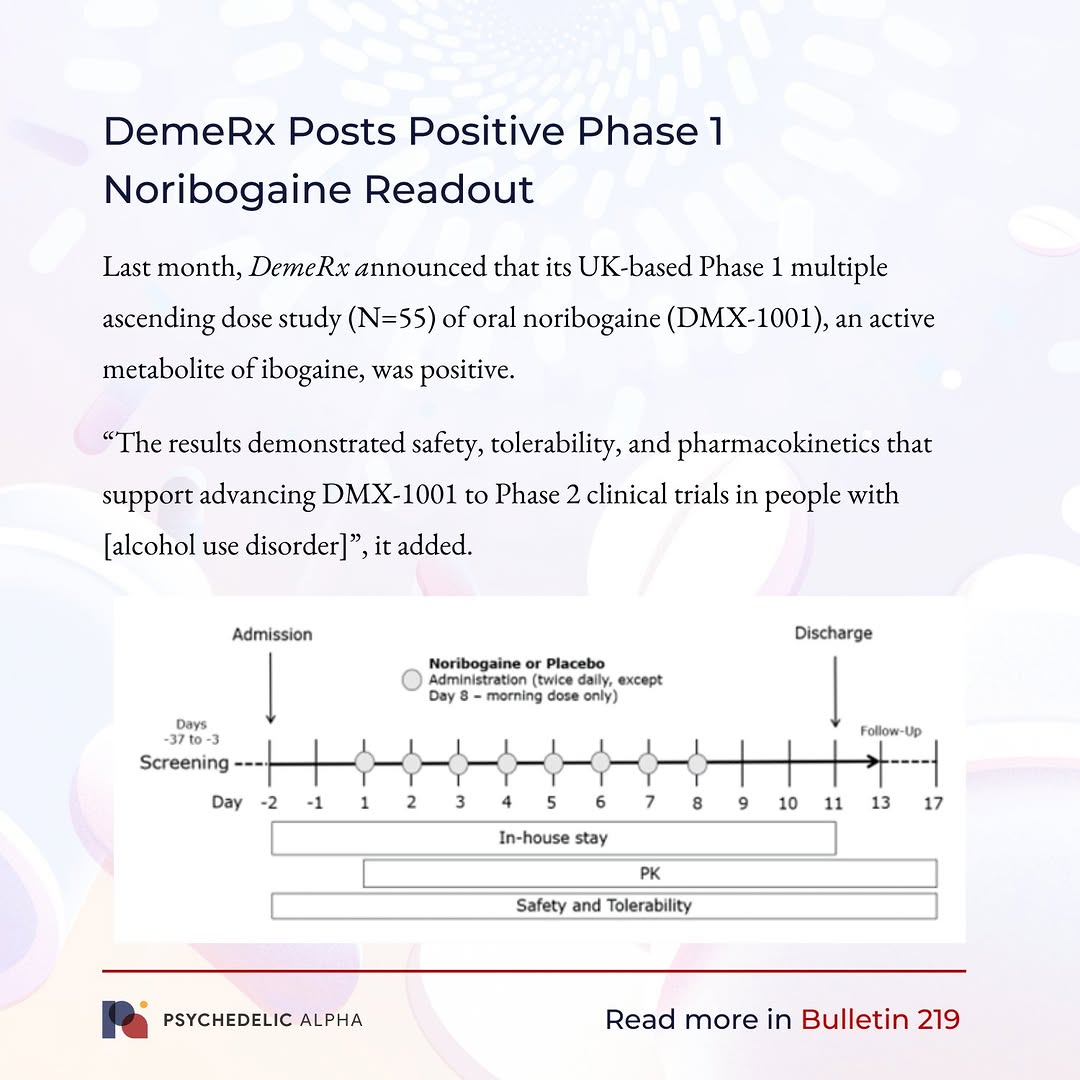
The significance: noribogaine in oral form showed acceptable safety and tolerability. This opens the path toward Phase 2 efficacy studies. If noribogaine can be delivered as a stable oral medication, it sidesteps many of the complications around ibogaine's current administration and metabolic variability.
The Ambio Parkinson's Case Study
Ambio Life Sciences, which operates a specialized center in Costa Rica, has published observational data on ibogaine treatment in individuals with Parkinson's disease and related conditions. One notable case involved a 43-year-old male with Parkinson's and neuropathic pain.
Ambio's observations documented improvements in motor control, pain, and functional capacity following treatment. This is not a randomized controlled trial—it's a single case observation. But it's significant because it shows what may be possible, and it drives interest in larger, more rigorous studies. Such real-world observations form the evidence foundation upon which next-generation clinical trials are built.
How Ibogaine May Help: Mechanisms
| Mechanism | How It May Help in Neurodegeneration | Status of Research |
|---|---|---|
GDNF Upregulation | Activates the brain's own neuroprotective repair pathways; may slow or arrest neuronal death | Preclinical evidence strong; early clinical observation promising |
Neuroplasticity Reactivation | Reopens the brain's capacity to form new connections and reorganize neural networks | Observational reports; proposed 90-day window remains area of active research |
Multi-Receptor Engagement | Acts across serotonin, dopamine, and glutamate systems rather than single pathway; may address complex neurodegenerative biology | Well-established pharmacologically; clinical implications still emerging |
Anti-Inflammatory Signaling | May reduce neuroinflammation, a key driver in Parkinson's, Alzheimer's, and other conditions | Theoretical and early preclinical; needs clinical validation |
Integration & Epigenetics | Profound experience may shift behavior, stress response, and lifestyle—gene expression follows behavior | Observed clinically; mechanistic study ongoing |
Conditions Being Explored
Ibogaine-assisted work is being explored (in research or clinical settings) for several neurodegenerative and brain-injury conditions:
Parkinson's Disease: Motor symptoms, dopamine dysregulation, neuropathic pain; case studies and case reports suggest potential benefit
Alzheimer's Disease and Dementia: Neuroinflammation and neurodegeneration; research is early but growing
Traumatic Brain Injury (TBI) and Post-Concussion Syndrome: Many veteran and athlete communities are watching this space closely
Multiple Sclerosis: Neuroinflammation and autoimmune aspects; limited data but emerging interest
Mild Cognitive Impairment: Potential to support cognitive reserve and slow progression
Important: These Are Emerging Areas
The evidence base varies significantly. Parkinson's has the most published case observations. Alzheimer's is largely preclinical. None of these constitute FDA-approved uses. Anyone considering ibogaine-assisted work for a neurodegenerative condition should: (1) consult a qualified neurologist; (2) understand their local legal and regulatory environment; (3) work with experienced, licensed medical professionals—never self-administer.
The Integration Equation: Medicine + Work
If the 90-day neuroplasticity window is real, then what you do in those 90 days is as important as the medicine itself. Research and clinical experience suggest a multi-modal approach:
Movement & Physical Therapy: Exercise upregulates GDNF and promotes neurogenesis. For neurodegenerative conditions, consistent, gentle movement—walking, swimming, tai chi, targeted physical therapy—appears crucial.
Nutrition: Ketogenic and anti-inflammatory diets have some supportive research in neurodegeneration. A skilled nutritionist familiar with brain health becomes a key collaborator.
Sleep & Circadian Health: The glymphatic system clears metabolic waste during deep sleep. Sleep quality directly influences neuroinflammation and GDNF expression.
Meditation & Mindfulness: These practices show measurable effects on brain structure and neuroinflammation markers in published research.
Cognitive Rehabilitation: Puzzles, language work, learning—the neuroplastic window is a chance to retrain and rebuild neural networks around areas of decline.
Community & Meaning: The subjective experience of connection, purpose, and hope influences immune function, inflammation, and healing capacity.
— Integrative neuroscience community reflectionNoribogaine is the biological key to neuroplasticity. It reopens the 'learning window' we had as children. But the key only opens the door. What you build beyond it is up to you.
What We Still Don't Know
Honest assessment matters. The ibogaine-neurodegeneration space is promising but not yet proven. Significant questions remain:
Optimal dose, timing, and frequency: Current evidence comes from diverse protocols. What's optimal for a 45-year-old with Parkinson's may differ from a 68-year-old with Alzheimer's—but we don't have that data yet.
Durability: Do benefits persist beyond the 90-day window? How many treatments may be needed across a disease course?
Predictors of response: Why do some people show significant improvements while others show modest changes? Genetics? Baseline disease stage? Integration quality? Unknown.
Mechanism confirmation: GDNF upregulation is a working hypothesis. Rigorous mechanistic studies in humans are needed.
Long-term safety: Ibogaine carries cardiovascular and liver considerations. Long-term safety in neurodegenerative populations requires more data.
Language Note
We use "may support," "research suggests," and "some users report" deliberately. This is not a clinical recommendation. Ibogaine remains a controlled substance in many jurisdictions. The emerging science is real, but it is early. The difference between hope and hype matters—especially for people and families facing progressive neurological disease.
The Researcher Behind the Science: Dr. Deborah Mash
Much of the scientific backbone in ibogaine-neurodegeneration research traces back to Dr. Deborah Mash, Professor Emeritus of Neurology at the University of Miami. Mash is a neuropharmacologist with decades of research on addiction, brain disorders, and neuroplasticity. She founded DemeRx specifically to advance noribogaine as a pharmaceutical candidate.
Mash's clinical experience in ibogaine administration and her neuroscience credentials give her work credibility—but also responsibility. She emphasizes that ibogaine is not a substitute for conventional care, only a potential adjunct to a comprehensive approach.
For the Person Facing Neurodegeneration
If you or someone you love is living with Parkinson's, Alzheimer's, TBI, or another neurodegenerative condition, you may have felt the narrowing of options. The standard medications work for a time, then plateaus. The condition progresses. The question "Is there anything else?" becomes louder.
Ibogaine is not a cure. It is not a miracle. But the emerging evidence suggests it may offer something: a reopening of plasticity, an activation of the brain's own repair capacity, a chance to arrest or slow decline when combined with dedicated integration work.
If you're exploring this path:
Consult qualified professionals—a neurologist familiar with neurodegenerative disease, and ideally a physician experienced in ibogaine-assisted work. Ask about DemeRx's clinical trials if applicable. Research accredited centers like Ambio if considering treatment.
Understand the legal landscape. Ibogaine is a controlled substance in many countries. In some jurisdictions, clinical research is underway. In others, it's available only in international settings. Know your situation.
Prepare for integration work. The medicine is one part. The 90 days after—movement, nutrition, meditation, cognitive work, meaning-making—may be where real change solidifies.
Connect with community. You are not alone in asking these questions. Veteran networks, patient advocacy groups, and online communities are exploring this territory carefully.
What's Next in the Research
The field is moving. DemeRx is planning Phase 2 trials with noribogaine in specific populations. Universities and research centers are investigating mechanisms. The Stanford Psychedelic Research Group, under researchers like Nolan Williams and others, has shown interest in brain-injury and neurodegeneration applications.
The next 2-3 years will likely bring:
- More published case observations from centers like Ambio and others
- Phase 2 efficacy data from DemeRx (timing uncertain; may be 2026-2027)
- Mechanistic studies diving deeper into GDNF, neuroinflammation, and circuitry
- Neuroimaging research showing PET, fMRI, and other markers before and after treatment
- Longer-term follow-up data from earlier cohorts, clarifying durability
These studies will not happen overnight. But the momentum is real. The questions are rigorous. The stakes are high. That combination tends to attract serious science.
— Adapted from clinical research community notesWe're honoured to have been featured in Neuro Rehab Times, highlighting research into neuroregenerative approaches. The intersection of neuroscience and patient experience is where real medicine lives.
A Final Word: Hope + Realism
Neurodegenerative disease is brutal. It takes time, agency, and identity. Desperation is rational. So is hope.
The evidence around ibogaine and neurodegeneration is not yet conclusive. But it is real. It is growing. It sits at the intersection of neuroscience, lived experience, and the simple human refusal to accept decline as inevitable.
If you're considering this path, move with eyes open. Demand evidence. Insist on qualified providers. Build your integration team. And honor the fact that you're not looking for magic—you're looking for a chance. That's honest. That's worth pursuing carefully.